- Xaña’s Marketing Gold
- Technology Today

Resolving Long-Standing Problems in a Full-Mouth Rehabilitation Case


Single-Visit Endodontics, Part 1: Are We There Yet?
Dentistry Today
- Share on Facebook
- Share on Twitter
Did you read the title of this article and think, “Single-visit endodontics? Of course, I’ve been doing it for years. What’s so new about that?” If you perform single-visit endodontics, you are part of the change in attitude—from never attempting a single visit to considering it common and routine. What has changed to make single-visit endodontics acceptable? Was it new techniques or was it simply driven by economics?
The fact that there is now widespread acceptance of single-visit endodontics for most vital cases represents significant progress. Until recently, this was not acceptable under any circumstances. But what about teeth with necrotic and infected pulps? In our view, single-visit endodontics is acceptable treatment in most cases, both vital and nonvital. This position is becoming more widely accepted and will continue. After all, when a canal is well cleaned at the first appointment, what more is there to do?
This article discusses the consideration of single-visit endodontics as the norm and not the exception. It also addresses (1) the economics of single visits, (2) when it is not wise to attempt single-visit treatment, (3) what research tells us about single visits, and (4) what an instrumentation technique must do to predictably improve the chances of success.
THE ECONOMICS OF SINGLE-VISIT ENDODONTICS
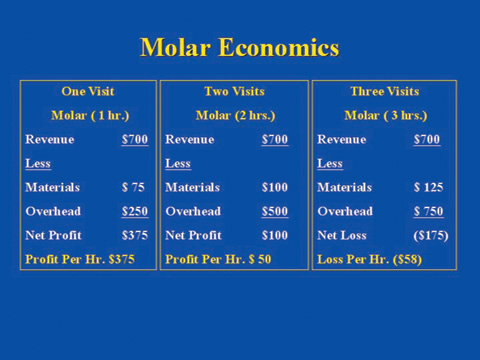
Based on economics, it is no surprise that single-visit treatment is becoming more widely accepted. Table 1 shows the economics of molar root canal treatment. With the fee remaining constant, regardless of the number of visits, there is a significant financial benefit for completing treatment in a single 1-hour visit because additional visits increase expenses, thereby reducing profits. A very profitable one-visit, 1-hour procedure becomes a loss when stretched to 3 visits. Assuming similar treatment results, patients also benefit. Dental visits, especially if not absolutely necessary, add an additional burden to their busy schedules.
THE BASICS OF SINGLE-VISIT ENDODONTICS
The basics of single visits were given to us in ENDO 101 and they are simple: make a correct diagnosis, clean the canal, and obturate it 3-dimensionally to prevent reinfection by the ever-present oral bacteria. We learned that the most important part of root canal treatment is to clean and disinfect the canal as well as possible. The basics have not changed at all.
To treat a tooth in one visit requires optimal cleaning and disinfection of the root canal system. Research tells us that this is accomplished most predictably when canal enlargement exceeds the diameter of the uninstrumented canal (mechanical cleaning), aided by the antimicrobial action of an irrigant (chemical cleaning). Infected tissue and bacteria located on canal walls and the superficial layer of dentinal tubules are removed by cutting away a thin layer of dentin. Any bacteria remaining deeper in the tubules are isolated by gutta-percha and sealer on the canal side and impervious cementum on the PDL side. Under these conditions, bacteria become inactive or die.
We disagree with the notion that single visits are not acceptable in infected cases and that medicaments must be used between appointments to kill all bacteria. There is a problem with this position because committing ourselves to removing all bacteria all of the time puts us in an untenable situation. We would have to remove an excessive amount of dentin to deal with bacteria deep in the tubules and find ways to deal with those located in lateral canals, apical deltas, fins, and isthmuses. Realistically, this is not possible in a clinical setting. This leaves medicaments the task of doing what is impossible to do with instrumentation, but we have no assurances that they will be effective in these “hard-to-get-to” places either. We advocate cleaning the main canal as best we can during the first visit and forgoing trying to do what is often impossible. If a thorough cleaning and canal sealing can be completed in the first visit, additional appointments don’t seem justified without clear evidence that patients will benefit.
APICAL DIAMETER AND APICAL ENLARGEMENT
To best clean the most important part of the canal (the apical part), instrumenting to the correct size is required. The size should not be determined by canal curvature nor should it be kept as small as possible. Additionally, it should not be based on what a root canal instrumentation system can or cannot do. Ideally, the apical part of the main canal should be prepared with instruments large enough to obtain a clean canal. Research clearly shows an inverse relationship between instrument size and the number of bacteria remaining in the canal. As instrument sizes increase, the number of bacteria decreases. Clearly, an undersized apical preparation compromises treatment.
To best illustrate the importance of apical diameter, let’s review 2 cases. Figures 1a and 2a show radiographs of failed root canal treatments. When one of this article’s authors (Dr. Wildey) re-treated the teeth, he found the canals underprepared apically. He re-treated them to larger sizes (using LightSpeed instruments), first gauging (sizing) the canals’ apical diameters, then using the instruments’ tactile feedback to arrive at the final apical preparation sizes. The larger sizes ensured cleaner canals and the lesions healed (Figures 1b and 2b). These 2 cases provide convincing clinical evidence that apical canal diameter and apical canal enlargement sizes are critical elements of successful endodontics.
EVALUATING QUALITY
How do we evaluate the quality of root canal treatment when it can be so subjective? We believe that the final apical preparation sizes achieved with root canal instrumentation are a major determinant of quality and should be routinely included when presenting a case. Just looking at aesthetically pleasing x-rays is not enough to conclude that a case is done well. After all, we all know that x-rays are only 2-dimensional, and that when a case looks bad, it is, but when it looks good, it may or may not be good. Having the apical preparation sizes of all canals can help us decide.
At a course sponsored by Loma Linda University (January 2003), Dr. Wildey demonstrated how instrument design can help determine the appropriate apical preparation size. He and 4 other well-known endodontists treated maxillary molars (live) while the audience watched on 3 large screens. After making straight-line access as described in an earlier article by Senia and Wildey,1 Dr. Wildey instrumented the canals using the LightSpeed technique2 and obturated them with SimpliFill.3
The final apical preparation sizes of the maxillary molar Dr. Wildey treated at Loma Linda were MB-1 and MB-2 = No. 55; DB = No. 55; and Palatal = No. 60. Obviously, all 4 sizes are larger than traditional sizes—not determined on a whim or a guess but dictated by the original canal diameter. Knowing final preparation sizes will help us evaluate the quality of treatment more objectively. We have to break the habit of evaluating quality of treatment just by looking at x-rays.
WHAT DOES THE LITERATURE SAY ABOUT CANAL SIZES?
Science and logic support the principle that larger apical preparations clean canals better, but how do we arrive at the correct size in a clinical setting? One can start by consulting the literature.4-8 Tables 2 and 3 show the data collected from various anatomical studies. Your first thought about the sizes shown in both tables may be that they are too large. However, before arriving at this conclusion, it’s important to know that the canals were not measured at the foramen or at the narrowest point. In general, they were made approximately 1 to 2 mm from the anatomic apex (coronal to the apical constriction). Compare your final apical preparation sizes with the sizes shown in the literature. If you are consistently smaller, there is a good chance you are underpreparing canals.
Since there is mounting evidence that “bigger is better,” what has been holding us back from giving apical canal diameter (the “forgotten dimension”) the importance it deserves?9 Why do we persist in believing that canals of molars can be thoroughly cleaned with instruments of size 25 or 30 when there is much evidence showing that this is not so? We believe past history provides the answer. Dentists learned that instrumenting curved canals with rigid stainless steel instruments larger than a No. 30 very often resulted in mishaps such as ledges, zips, perforations, and blocked canals. The choice was easy: instrument only with the smaller sizes or expect to have some problems.
Flexible instruments made of nickel titanium (NiTi) now make it possible to safely instrument to larger apical sizes. However, proceed with caution. NiTi instruments can still transport and ledge canals, particularly with increasing tip sizes and tapers. Instrument design that takes maximum advantage of the material is a factor that should be considered.
BIGGER IS BETTER
“Bigger is better” means instrumenting apical canals to the correct size, a size that is usually larger than traditionally accepted. It means that bigger instruments are required to clean the canal 3 to 5 mm coronal to the constriction where the canal diameter is considerably larger than that of the constriction. Bigger is better does not apply to the apical constriction. The apical constriction, when present, is the narrowest part of the canal and should be instrumented (if desired) to a size just slightly larger than its existing “natural” diameter. And finally, bigger is better certainly does not mean over-instrumenting canals and subjecting roots to possible fracture. Because most of the chewing forces are concentrated coronally, a slight over-enlargement of the apical third of the canal (if it occurs) should not be clinically significant.
Our goal is larger and cleaner canals apically without removing excessive dentin coronally. This can be accomplished by using a flexible material (NiTi), a flexible noncutting shaft, and a short blade with a noncutting pilot tip. In the authors’ opinion, this design is best suited to follow the canal. Practitioners have been conditioned to believe that apical canal sizes are small even when research shows otherwise (Tables 2 and 3). If skeptical about the sizes given, we ask you to look at the very tip of instruments, sizes 20 through 35, then ask yourself if canals are really that small. Most likely you will appreciate just how small these sizes really are and intuitively accept the fact that apical canals are larger in most cases.
BEING COMFORTABLE WITH SINGLE VISITS
We would like to make it clear that even though we believe in the concept of single-visit treatment, there are certain exceptions. We avoid single visits when the following conditions are present: (1) cellulitis, (2) acute apical abscess requiring incision and drainage, (3) severe pain when the tooth is lightly touched, (4) a weeping canal that cannot be dried, and (5) difficult cases that extend beyond our allotted time and the patient’s tolerance.
To be comfortable with single-visit treatment requires an understanding of when it is not a good idea and the manner in which the major elements of root canal treatment influence success and failure. The 2 major components of canal instrumentation are working length and final apical preparation size (canal diameter). Let’s discuss their role in single-visit endodontics.
Working Length: Must It Be Perfect or Is There a Biological Tolerance?
Let’s look at the case shown in Figure 2 again and examine how it relates to working length. The pretreatment x-ray (Figure 2a) shows both mesial canals ledged and obturated short. Upon re-treatment, Dr. Wildey was unable to bypass the ledges, resulting in a working length very similar (short) to the treatment that failed. Even though the mesial canals were re-obturated short because of the ledge, the lesion healed (Figure 2b). This strongly suggests that a “biological tolerance” exists for working length if canals are well-cleaned and sealed. Our highly effective body defense system can promote healing even when the working length is not ideal.
Let’s further discuss working length. Where is the ideal working length in relation to the apical foramen? Is the ideal length slightly beyond the foramen, flush with the foramen, or 0.5 to 1.0 mm short of the foramen? (Since the apical foramen marks the end of the root canal, working lengths can be more precisely located when referenced to the foramen rather than the apex.) What working length will ensure greater success given the same quality of canal instrumentation and obturation? There is abundant clinical and research evidence to support that there is a biological tolerance for working length. In other words, the ideal length is not always possible to achieve, but if you are a little long or a little short, there is no convincing evidence that the case will fail just because of this.
Canal Diameter: Must It Be Perfect or Is There a Biological Tolerance?
Does the same “biological tolerance” for working length also hold true for canal diameter? Before answering, it should be pointed out that canal diameter is often considered the “forgotten dimension” of a 3-dimensional root canal system. A review of the literature reveals that much has been written about length control but very little about diameter control. This implies that many believe getting the working length correct is what matters most. But, in a 3-dimensional environment, the existing (preinstrumentation) canal size is a very important factor. If canal size is not considered during instrumentation, then exactly how can one accurately determine when instrumentation has achieved a clean canal?
Can the body’s defense system cope successfully with a debris-filled, infected canal resulting from a size 25 master apical instrument being used in a size 50 canal? Figure 3 compares the cross sectional area of a root canal prepared to a No. 50 file with that of a No. 25 file. While it seems intuitive that the area cleaned by a No. 50 is twice as much as a No. 25, the area of the canal cleaned is actually 4 times larger! This is why a few instrument sizes smaller than the “ideal” size result in a large amount of underpreparation and why emphasis should be placed on instrumenting to the correct size.
Our opinion is that there is little biological tolerance for apical preparation size with necrotic cases. The molar in Figures 4a and 4b is a good example. It failed even though it had been instrumented and obturated to acceptable working lengths (Figure 4a). When re-treated with similar working lengths but with larger apical preparations (mesials = No. 50; distal = No. 60), healing of the rather extensive lesion took place (Figure 4b). Underpreparation, as demonstrated in this case, results in a continuous battle between the periradicular tissues and bacteria and their toxins. The body’s defense mechanism is now dealing with a very different situation as compared to working length. When working length is not ideal but everything else is done correctly, there is no continuous battle. The bacteria are isolated, and in a well-cleaned and sealed canal, there is no apical recontamination. Apical underpreparation results in debris and bacteria remaining in the canal, making isolation with the obturation virtually impossible.
1 OR 2 APPOINTMENTS?
When canals are cleaned and disinfected at the first appointment, why not complete treatment at that time? Is there reason to expect a higher success rate with a second visit when a biologically acceptable level of cleanliness is attained at the first one? Wouldn’t delaying completing treatment until the second visit perhaps be counterproductive given the possibility of recontamination between visits? Let’s look at the science to answer some questions and help us decide.
The Science of Single-Visit Endodontics: Apical Sizes Revisited
Recent studies support larger apical preparation sizes to remove more infected tissue and bacteria10-13 and provide more canal space for more effective irrigation.14 Simply stated, preparing canals to larger apical sizes is the right thing to do, especially if single-visit endodontics is our goal.
More than 25 years ago, Kerekes and Tronstad provided evidence that root canals are much larger than once thought.4-6 Many years have passed, yet the myth remains that apical canals are very small and that instrumentation need only be to sizes No. 20 to 35 in most canals. More recent studies show otherwise.7,8,15 There are always exceptions, but they are the exception, not the rule.
Shuping et al11 found that molar canals prepared to a No. 36 or No. 46 with 0.04-taper NiTi instruments rendered only 61.9% of the canals bacteria-free even after irrigation with NaOCl. Their study concluded that larger apical preparations are required for better debridement and to give irrigants better access to the apical region. The investigators also noted that if a canal is not instrumented to an appropriate size, the purpose of using an antibacterial irrigant might be negated. Their findings certainly do not make a good case for single- visit endodontics when canals are underprepared.
Siqueira et al12 found that canals prepared to a No. 20 with 0.12-taper NiTi instruments resulted in only 66.5% of the specimens being bacteria-free. They stated that large preparations incorporate more anatomical irregularities and allow the removal of a substantial number of microbial cells from the root canal. They also mentioned that effective irrigation might not occur consistently unless the canals are sufficiently enlarged and that larger preparations may enhance the effects of irrigation in the apical third.
Rollison, Barnett, and Stevens13 prepared canals to No. 35 with 0.04-taper instruments and compared them with canals prepared with No. 50 0.02-taper instruments. They concluded that the 0.02-taper No. 50 instruments removed significantly more bacteria than the 0.04-taper No. 35 instruments. This study further demonstrates that apical preparation size really does matter.
Peters and Barbakow14 concluded that a larger canal preparation enabled more effective irrigation to remove the smear layer and debris. Card et al10 theorized that instrumenting canals to larger apical sizes would result in a significant reduction of canal bacteria and their study supported this theory. Canal preparation sizes ranged from No. 80 to No. 100 in cuspid and premolar canals and No. 60 in molar canals (using the LightSpeed system). The researchers concluded that a high percentage of infected canals would no longer harbor cultivatable bacteria when instrumented to the sizes used in their study. They also stated that with many teeth, this regimen may be a substitute for a 2-stage procedure utilizing an intracanal dressing between visits.
Taken together, these studies clearly indicate that as apical enlargement increases, the number of intracanal bacteria decreases. Is a figure of 89% to 100% reduction of intracanal bacteria, as determined by Card et al,10 good enough to justify single-visit endodontics? We believe it is. After all, there are no assurances that extending treatment to 2 or more visits will ensure a higher success rate, especially when canals are not well-cleaned.
ROLE 0F OBTURATION AND IRRIGATION
Successful single-visit treatment depends on effective mechanical debridement, chemical disinfection, and proper sealing of the canal system. Obturation can only be as good as the instrumentation, since filling material cannot occupy the same space as the debris left by poor instrumentation.
Effective irrigation can only be as good as the space available allows. A narrow, confined space inhibits a free exchange of irrigant. Larger apical preparations, so essential for canal disinfection and removal of debris, also enhance the action of irrigants. Since irrigation with pressure should never be used, larger preparations allow irrigating solutions to be placed closer to working length with added safety—another benefit and another reason that supports the idea that bigger is better.
Times have changed and new technology has given us instruments with better designs and materials. Numerous studies have shown that when flexible instruments are used, instrumenting to larger apical sizes produces minimal or at least not clinically relevant canal transportation. Yes, NiTi rotary instrumentation is a welcome change, and most dentists who have made the transition successfully wouldn’t want to go back to hand filing.
The ability of new rotary systems to reduce treatment time puts single visits within reach of most practitioners and prompts us to take another look at a concept that makes a lot of sense. But just because NiTi rotary systems are faster than hand instrumentation, this alone cannot justify single-visit endodontics. In this article, we tried to give valid, scientifically supported reasons for single-visit root canal treatment. Are we there yet? Think about it—and you decide.
Acknowledgment
The authors want to thank Mr. Steven S. Senia, BSIE, MBA, for his contributions to this article.
1. Senia ES, Wildey WL. “Straight-line” access: a must for faster and better endodontics. Dent Today . 2003;22:40-45.
2. The LightSpeed and SimpliFill Technique Guide . San Antonio, Texas: LightSpeed Technology Inc; October 2002.
3. Wildey WL, Senia ES. Simple, precise, and predictable root canal obturation. Dent Today . 2002;21:60-65.
4. Kerekes K, Tronstad L. Morphometric observations on root canals of human anterior teeth. J Endod . 1977;3:24-29.
5. Kerekes K, Tronstad L. Morphometric observations on root canals of human premolars. J Endod . 1977;3:74-79.
6. Kerekes K, Tronstad L. Morphometric observations on the root canals of human molars. J Endod . 1977;3:114-118.
7. Gani O, Visvisian C. Apical canal diameter in the first upper molar at various ages. J Endod . 1999;25:689-691.
8. Sabala CL, Biggs JT. A standard predetermined endodontic preparation concept. Compendium . 1991;12:656-663.
9. Senia ES, Wildey WL. Canal Diameter: The Forgotten Dimension. Dent Today . 2001; 20: 58-62.
10. Card SJ, Sigurdsson A, Orstavik D, et al. The effectiveness of increased apical enlargement in reducing intracanal bacteria. J Endod . 2002;28:779-783.
11. Shuping GB, Orstavik D, Sigurdsson A, et al. Reduction of intracanal bacteria using nickel-titanium rotary instrumentation and various medications. J Endod . 2000;26:751-755.
12. Siqueira JF Jr, Rjcas IN, Santos SR, et al. Efficacy of instrumentation techniques and irrigation regimens in reducing the bacterial population within root canals. J Endod . 2002;28:181-184.
13. Rollison S, Barnett F, Stevens RH. Efficacy of bacterial removal from instrumented root canals in vitro related to instrumentation technique and size. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2002;94:366-371.
14. Peters OA, Barbakow F. Effects of irrigation on debris and smear layer on canal walls prepared by two rotary techniques: a scanning electron microscopic study. J Endod. 2000;26:6-10.
15. Wu MK, R’oris A, Barkis D, et al. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod . 2000;89:739-743.
Dr. Senia has been published in national and international journals. He is a diplomate of the American Board of Endodontics, a former member of The Journal of Endodontics editorial board and a consultant for the NASA space program. After receiving both his BS and DDS degree from Marquette University in 1963, he reentered the US Air Force (he had prior service as a pilot) to take a GPR residency program at Chanute Air Force Hospital. In 1969, he received a certificate in endodontics and a master of science degree from The Ohio State University. He retired from the US Air Force in 1981 as a colonel and as chairman of endodontics at Wilford Hall Medical Center and accepted the position of director of the endodontic postdoctoral program at the University of Texas Dental School at San Antonio. He retired in 1992 as a professor and presently holds the title of clinical professor at the university.
Disclosure: Dr. Senia is the co-inventor of the LightSpeed root canal instrumentation and SimpliFill obturation systems.
Dr. Wildey is presently in an endodontic practice in the Dallas/Ft. Worth area. He earned his DDS degree from Georgetown University in 1976 and after graduation served 4 years as a general dentist in the US Air Force. In 1988, he received a certificate in endodontics from the University of Texas Dental School at San Antonio. He can be reached at [email protected] .
Disclosure: Dr. Wildey is the co-inventor of the LightSpeed root canal instrument and SimpliFill obturation systems.

Related Articles

Seeing Endodontics Through a New Lens: Fueling Innovation to See Dentistry’s Darkest Side

Principle-Guided Endodontic Treatment

Common Sense Insights Into Present-Day Endodontic Instrumentation Techniques
Recent Posts

Dr. Ross Nash Full Mouth Reconstruction Course Coming to New Jersey for the First Time

Discover the Future of Dentistry with Sage Dental

Massachusetts Dental Society Names “10 Under Ten”
- Submissions
- Privacy Policy

IP Indian Journal of Conservative and Endodontics
Official Publication of Khyati Education And Research Foundation
Published by IP Innovative Publication Pvt. Ltd.

Journal Information
Journal ID ( nlm-ta ): Innovative Publication
Journal ID ( publisher-id ): Innovative Publication
Journal ID ( journal_submission_guidelines ): https://www.innovativepublication.com/journal/IJCE
Title: IP Indian Journal of Conservative and Endodontics
ISSN: 2581-8988
Article Information
Copyright: 2021
Date received: 29 August 2021
Date accepted: 15 September 2021
Publication date: 25 September 2021
DOI: 10.18231/j.ijce.2021.032
Single visit endodontics
[ 0000-0003-2165-4524 ] R. Geethanjali [ 1 ]
Email: [email protected]
Designation:
P G Student
[ ] Naveen kumar [ 1 ]
[ ] K Madhuram [ 1 ]
Professor & HOD
[ ] Ashok Leburu [ 1 ]
Dept. of Conservative Dentistry and Endodontics, Karpaga Vinayaga Institute of Dental Science Kanchipuram, Tamil Nadu India
A successful endodontic treatment depends upon localization, proper chemo mechanical preparation of the root canal system, debridement, shaping, disinfection, and three-dimensional obturation of canal system. To achieve this, endodontic therapy used to be performed in multiple visits for complete disinfection of the canals in other words for the better success of endodontic therapy.1
Introduction
A successful endodontic treatment depends upon localization, proper chemo mechanical preparation of the root canal system, debridement, shaping, disinfection, and three dimensional obturation of canal system. To achieve this, endodontic therapy used to be performed in multiple visits for complete disinfection of the canals in other words for the better success of endodontic therapy. 1 One-visit endodontic therapy is defined as ‘the conservative non-surgical treatment of an endodontically involved tooth consisting of complete biomechanical cleansing, shaping and obturation of the root canal system during one visit’. 2 The concept of single visit root canal treatment is predicted on the entombing theory, 3 which states that the large number of microorganisms are removed during cleaning and shaping 4 , 5 and therefore the remaining bacteria are entombed by the root canal obturation, and it’ll miss the essential elements to survive; nutrition and space. 6 , 7 The recent advances, helps the dental practitioners and endodontists to perform the root canal treatment in single visit.
Selection criteria for single visit endodontics
Oliets c riteria 8, positive patient attitude.
Patient should be cooperative and prepared for single visit endodontics. Noncooperative patients with TMJ problems, limited mouth opening should be avoided for single visit endodontics
Sufficient time to complete procedure
Absence of acute symptoms requiring drainage through the canal and of persistent continuous flow of exudate or blood.
Absence of anatomic obstacles like calcification in the canals and procedural difficulties (ledge formation, blockage, perforation, inadequate fills).
Indications
Uncomplicated vital teeth
Physically compromised patient
Medically compromised patients
Fractured anterior where esthetics is a concern
Apprehensive but cooperative patient
Uncomplicated non vital teeth with sinus tract
Contraindications
Teeth with anatomic anomalies for e g calcified and curved canals
Patients with allergies or previous flare ups
Acute alveolar abscess cases with presence of pus discharge
Patients who cannot keep mouth open for long duration (TMJ disorders
Symptomatic non vital teeth and presence of no sinus tract
Asymptomatic non vital teeth with presence of periapical pathology
Patients who have acute apical periodontitis with severe pain on percussion
Teeth with limited access
Patient comfort
Minimizes fear and anxiety
Familiarity of the canal anatomy
Reduced intra appointment pain
Restorative consideration
Disadvantages
Tiring for patient
Extremely fine, calcified, multiple canals cause stress for both the patient and the clinician
Inexperienced clinicians
Single Visit Endodontic Therapy: Acceptence
Healing rate, post operative healing.
Healing processing after any endodontic therapy will usually occur following an accurate diagnosis, proper case selection and the use of skilled techniques of treatment. These procedures are based upon known biological principles incorporated into the technique triad namely biomechanical preparation of the canal system, debridement and disinfection and complete obturation of the prepared canals. All of these objectives must be achieved in order to ensure a successful procedure. 9 In many studies it was found that there was no significant difference in healing rate between single and multiple-visit root canal treatment in teeth with infected root canals (80.1% vs 80.0%).
The short‑ or long‑term follow‑up of the bone radiographic image and size of the lesion is the most commonly used technique to evaluate the healing, usually based on the PAI score developed by Orstavik et al. 10 , 11
PAI 1: normal periapical structure are seen
PAI 2: small changes in the bone structure not a specific characteristic of apical periodontitis
PAI 3: changes in the bone structure with mineral loss characteristic feature of apical periodontitis
PAI 4: well-defined apical radiolucency seen
PAI 5: severe periodontitis with exacerbating features and bone expansion are evident
Endodontic flare-up and pain
The American association of endodontists defines an endodontic flare-up as an acute exacerbation of an asymptomatic pulp or periapical pathosis after the initiation or continuation of root canal treatment.
The etiology for flare ups are numerous and often multifactorial. Dr. Seltzer 12 proposed a number of hypotheses, some of which may be interrelated. They include:
Microbial factors
Change in periapical tissue pressure
Local adaptation syndrome alteration
Effects of chemical mediators
Immunological phenomena
Psychological factors
Flare-ups are caused when microbial toxins get extruded beyond apical foramen causing acute inflammatory response. This usually happens during either over instrumentation or over obturation. Its prevalence ranges between 3 and 58 percent. 13 Postoperative pain occurs mainly due to acute inflammation in the periradicular tissue caused by the penetration of microorganisms from the root canal during endodontic retreatment. 11 Postoperative pain depends upon number of visits as well as preoperative factors, preoperative complications, the periapical index (PAI) score, the size of the radiolucency, the quality of the coronary restoration, intraoperative factors, the intracanal medications, tooth localization, inadequate instrumentation, extrusion of intracanal medicament, age, sex, periapical pathosis, and apical debris extrusion and irrigants extrusion. 14 , 15
During the treatment, debris comprising of necrotic tissue, bacteria and their products are commonly pushed into the periapical area which leads to inflammation or exacerbation of previously present inflammation, resulting in post endodontic pain. Teeth that had non-vital pulp before treatment were associated with a significantly greater occurrence of post-obturative pain. The reason for longer duration of pain with manual instrumentation could be because of higher debris load in the periapical area as a result of piston like effect generated with manual instrumentation.
Pain relief in case of over-instrumentation is often dependent on an analgesic strategy. The under-instrumented case may require further instrumentation to the correct measurement as well as analgesic. Another study reported that a combination of calcium hydroxide and chlorhexidine intracanal medications was recommended to reduce postoperative pain with preexisting symptoms, in retreatment cases. Nonsteroidal anti-inflammatory drugs (NSAIDs) have been shown to be effective for managing pulpal and periapical pain. However due to renal effects of NSAIDs as well as interactions with many anti-hypertensive drugs, acetaminophen should be considered for post treatment pain in patients with known sensitivity to NSAIDs or aspirin. Pretreatment with NSAIDs for irreversible pulpitis should have the effect of reducing pulpal levels of the inflammatory mediator prostaglandin E2 (PGE2).
Pain Management
Pain management in endodontics depends on the accurate diagnosis of the cause of the pain. The methods by which an accurate diagnosis can be made are: 16
Clinical examination
Periapical testing
Pulp testing
Radiographic examination
The practitioner must be able to differentiate Odontogenic pain from non-odontogenic pain
Ideal endodontic therapy would eliminate all pain that exists in the involved tooth. But, the physiodynamics of the inflammatory process do not allow pain to immediately disappear once the source of the pain is eradicated.
An acute inflammatory process causes increase in the hydrodynamic pressure in periodontal ligament space, resulting in a pain response. This inflammatory process may arise during the root canal procedure. These include hemorrhage resulting from pulpal extirpation, cleaning and shaping of the root canal systems, irrigation, intracanal medications and/or root canal obturating materials. Any kind of Injury to the periradicular tissue initiates the inflammatory cascade. Inflammatory mediators; histamine, serotonin, bradykinin, prostaglandin, and leukotriene are released, causing increased vascular permeability and eventually pain.
The main function of analgesic use is pain relief. Nonsteroidal anti-inflammatory drugs inhibit the synthesis of prosthaglandin by decreasing the activity of the enzyme cyclooxygenase, which results in decreased formation of prostaglandin precursors. Prophylactic oral administration of NSAIDs before RCT can block the cyclo oxygenase pathway and by this application, the pain sensation can be blocked even before it begins. researchers have showed that preoperative administration of NSAIDs cause decrease in pain level at the initial hours after RCT. By administering NSAIDs prior to root canal therapy, the cyclo-oxygenase pathway can be blocked and the pain sensation can be prevented before it even begins. 17
It should be considered adjunctive drugs that act to enhance overall analgesia at the cost of increased adverse effects.
Corticosteroids
It can be used in specific situations where the pain is inflammatory in origin, where there is no infection and where there are no contraindications to the chosen drug being used, like emergencies (adrenal crisis, anaphylaxis and allergic reactions), severe post-operative swelling, following severe trauma, periapical nerve sprouting and acute apical periodontitis following removal of an acutely inflamed pulp and for some oral ulcerations, mucosal lesions that cannot be managed with topical medications. 18 In endodontics the importance of drug administration can be explained by three phases: pre-operative, intra-operative and post-operative. Pre-operative pain management involves administration of local anaesthesia and prophylactic medication. Some patients report with a hot pulp (dental pulp that does not respond to local anesthesia), wherein premedication with specific NSAIDs may be required.
Single visit endodontics vs multiple visit endodontics:
The two basic parameters used for the comparison of single-visit and multiple-visit endodontic therapy are:
Incidence of post-operative pain and flare-ups
Success versus failure rates
Post-operative pain.
Fear of post-operative pain following treatment is the biggest factor in avoiding single-visit endodontic therapy. A various number of studies and research have been done to compare the incidence of post-operative pain in single- versus multi-visit endodontic therapy. Although a number of studies in various literature showed that there is no significant difference between the two treatment protocols as far as incidence of post-operative pain is considered, there is a lack of evidence-based data to reinforce this. 19 , 20
This can be attributed to following reasons
The difference in criteria included (vital versus non-vital), variability in sample size, subjective nature of the pain interpretation and evaluation, and pre-operative symptoms of patients (with or without preoperative pain) patients’s anxiety regarding the treatment can alter the incidence of reported pain experience
Endodontic success indicators can be evaluated as short term or long term. The short-term indicators concern the absence of any postoperative discomfort.Long-term success of any treatment is dependent on various criteria, including case selection, treatment procedures and protocols, time management and sufficient duration of recall appointments. Long time success is based mainly on the healing of periapical lesions whenever present, and the prevention of new lesion.
Most of the studies in various literature indicate that there is minor or no substantial difference in the success rates of single- and multiple-visit endodontic therapy. A study by Jurcak et al reported 89% success rate following single-visit endodontic therapy. Despite Soltanoff’s report of considerably more pain in association with single-visit endodontic treatment, he found that both techniques provided success rates exceeding 85%. According to Peters and Wesselink, 21 complete radiographic healing was observed in 81% of the cases treated in one visit and 71% of the cases treated in two visits. Overfilling has been identified as a factor associated with a lower success rate (Sjogren et al.1990). 22 The teeth in which there was evidence of the periapical extension of pulpal disease had significantly higher incidence of failure. There was also higher incidence of failure in those teeth that were retreated endodontically.
A retrospective study by Field et al. 23 concluded that no statistically significant differences were observed between the two treatment protocols based on gender, age, arch or provider. However, they proposed that anterior teeth were more successful than posterior teeth. This was in accordance with the findings of Rudner and Oliet. 24 This difference is mostly due to the anatomical variations of posterior teeth. On the contrary. Similarly, a comparable percentage of radiographic healing was seen in both the treatment protocols but the Ca(OH)2 group (multiple-visit) showed fewer failed and more improved cases.
The reasons for differences in the percentage of success and failure rates in studies and opinion among the researchers can be due to: 25 , 26 , 27
The original investigators in their research did not treat acutely infected or abscess teeth in a single visit.
Lack of good unbiased studies that can be used for clinical decision making
Due to the difference in the definition of success as proposed by different authors, the success of an endodontic treatment is often poorly define. Variables such as, the skill of operators, appropriate diagnosis, proper case selection, reviewing radiographs, the techniques and materials used, and the time frame of the treatment can also determine the results.
With the advent of technological advancement and emergence of new devices, evidence-based dentistry and more scientific deliberations and the concept of maximum dentistry in minimum visits led to popularity towards various protocols to enable dentists to venture into single visit endodontics with reasonable level of outcome. Single visit root canal treatment versus the multiple visit root canal treatment has been the subject of a long-standing debate within the dental community, when the clinicians have to decide the choice of treatment, the central issues that should be considered are effectiveness, complication, cost and probably patient/operator satisfaction.
The case selection should be done properly and thorough adherence to standard endodontic principles, with no shortcuts, results in successful single-appointment endodontics. Practitioners should attempt single-visit root canal treatment only after making an honest assessment of their endodontic skills, training, and ability.
Source of Funding
Conflict of interest.
F Ahmed N Thosar M S Baliga N Rathi single visit endodontic therapy: A reviewAustin J Dent2016321035
P J Ashkenaz One-visit endodonticsDent Clin North Am198428485363
L B Peters P R Wesselink W R Moorer The fate and the role of bacteria left in root dentinal tubulesInt Endod J199528295104 10.1111/j.1365-2591.1995.tb00166.x
G Shuping D Orstavik A Sigurdsson M Trope Reduction of intracanal bacteria using Nickel-titanium rotary instrumentation and various medicationsJ Endod200026127516 10.1097/00004770-200012000-00022
B C Dalton D Orstavik C Phillips M Pettiette M Trope Bacterial reduction with nickel-titanium rotary instrumentationJ Endod1998241176370 10.1016/S0099-2399(98)80170-2
W Soltanoff A comparative study of the single-visit and the multiple visit endodontic procedureJ Endod19784927881 10.1016/s0099-2399(78)80144-7
R Weiger R Rosendahl C Lost Influence of calcium hydroxide intracanal dressings on the prognosis of teeth with endodontically induced periapical lesionsInt Endod J200033321945 10.1046/j.1365-2591.1999.00298.x
S Oliet Single-visit endodontics: a clinical studyJ Endod19839414752 10.1016/S0099-2399(83)80036-3
S Oliet Single-visit Endodontics: A Clinical StudyJ Endod19839416
D Orsravik K Kerekes H M Eriksen The periapical index: A scoring system for radiographic asessment of apical periodontitisEndod Dent Traumatol1986212034 10.1111/j.1600-9657.1986.tb00119.x
V Petrovic V O Galic Postoperative pain after primary endodontic treatment and retreatment of asimptomatic teethStomatoloski glasnik Srbije 20115827581 10.2298/SGS1102075P
S Seltzer I J Nadirof Flare-ups in Endodontic: I. Etiological factorsJournal of Endodontics198511472478
E Gondim Postoperative pain after the application of two different irrigation devices in a prospective randomized clinical trialJ Endodontics201036812951301 10.1016/j.joen.2010.04.012
S Shahi V Asghari S Rahimi Postoperative Pain after Endodontic Treatment of Asymptomatic Teeth Using Rotary Instruments: A Randomized Clinical TrialIran Endod J 20161113843 10.7508/iej.2016.01.008
M H Nekoofar M S Sheykhrezae N Meraji Comparison of the effect of root canal preparation by using Wave One and ProTaper on postoperative pain: a randomized clinical trialJ Endod201541557583 10.1016/j.joen.2014.12.026
T Nivethithan J D Raj Endodontic pain-cause and management: a reviewInt J Pharm Sci Res6727237 10.13040/IJPSR.0975-8232.6(7).2723-27
J R Vane Y S Bakhle R M Botting Cyclooxygenases 1 and 2Annu Rev Pharmacol Toxicol19983897120 10.1146/annurev.pharmtox.38.1.97
R A Seymour J G Meechan M S Yates Pharmacology and Dental Therapeutics7th 1999568
C Sathorn P Parashos H Messer The prevalence of postoperative pain and flare-up in single- and multiple-visit endodontic treatment: a systematic reviewInt Endod J2008412919 10.1111/j.1365-2591.2007.01316.x
L Figini G Lodi F Gorni M Gagliani Single versus multiple visits for endodontic treatment of permanent teethCochrane Database Syst Rev 20071745296 10.1002/14651858.CD005296.pub2
L B Peters P R Wesselink Periapical healing of endodontically treated teeth in one and two visits obturated in the presence or absence of detectable microorganismsInt Endod J20023586607 10.1046/j.1365-2591.2002.00541.x
U Sjogren B Hugglund G Sundqvist K Wing Factors affecting the long-term results of endodontic treatmentJ Endod19901610498504 10.1016/S0099-2399(07)80180-4
S Oliet single-visit endodontics: A clinical study.journal of endodonticsJ Endod19839414752 10.1016/S0099-2399(83)80036-3
W L Rudner S Oliet Vassor R, Operating microscope in endodontics: A systematic reviewOpen J Stomatology19812215
J Fox J S Atkinson A P Dinin E Greenfield E Hechtman C A Reeman Incidence of pain following one-visit endodontic treatmentOral Surg Oral Med Oral Pathol197030112330 10.1016/0030-4220(70)90021-6
I Wolch The one-appointment endodontic techniqueJ Can Dent Assoc197541116135
W Soltanoff A comparative study of the single-visit and the multiple-visit endodontic procedureJ Endod19784927881 10.1016/s0099-2399(78)80144-7
Categories:
Subject: Review Article
Endodontics
jats-html.xsl
© 2021 Published by Innovative Publication Creative Commons Attribution 4.0 International License (creativecommons.org)
© This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Table details
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License , which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
- Current Issue
Volume: , Issue:
- Article highlights
- Article tables
- Article images
Article History
Received : 29-08-2021
Accepted : 15-09-2021
Available online :
View Article
PDF File Full Text Article
Copyright permission
PDF File XML File ePub File
Digital Object Identifier (DOI)
Article Metrics
Share article, citation managers.
Download Citation
Bookmark article
Article Indexing
Article statistics
Article access statistics.
Viewed: 3444
PDF Downloaded: 3224
- General Information
- Manuscripts Submission
- Manuscript Submission Checklist
- Plagiarisms
- Cover Letter
- Copyright Declaration
- Publication Charges
- Contributors Confirmation
- Editorial Process
- Conflicts Of Interest
- Advertisement
- Peer Review Process
- Manuscript Submission Steps
- Submit Manuscript
- Author Editing Services
- Call For Paper For Upcoming Next Issue
- Join Reviewer | Editorial Board
- Advertisement Policy
- Editorial Board
- Reviewer Board
- About Journal

Single-visit or multiple-visit root canal treatment: systematic review, meta-analysis and trial sequential analysis
Affiliation.
- 1 Department of Operative and Preventive Dentistry, Charité-Universitätsmedizin Berlin, Berlin, Germany.
- PMID: 28148534
- PMCID: PMC5293988
- DOI: 10.1136/bmjopen-2016-013115
Objectives: Single-visit root canal treatment has some advantages over conventional multivisit treatment, but might increase the risk of complications. We systematically evaluated the risk of complications after single-visit or multiple-visit root canal treatment using meta-analysis and trial-sequential analysis.
Data: Controlled trials comparing single-visit versus multiple-visit root canal treatment of permanent teeth were included. Trials needed to assess the risk of long-term complications (pain, infection, new/persisting/increasing periapical lesions ≥1 year after treatment), short-term pain or flare-up (acute exacerbation of initiation or continuation of root canal treatment).
Sources: Electronic databases (PubMed, EMBASE, Cochrane Central) were screened, random-effects meta-analyses performed and trial-sequential analysis used to control for risk of random errors. Evidence was graded according to GRADE.
Study selection: 29 trials (4341 patients) were included, all but 6 showing high risk of bias. Based on 10 trials (1257 teeth), risk of complications was not significantly different in single-visit versus multiple-visit treatment (risk ratio (RR) 1.00 (95% CI 0.75 to 1.35); weak evidence). Based on 20 studies (3008 teeth), risk of pain did not significantly differ between treatments (RR 0.99 (95% CI 0.76 to 1.30); moderate evidence). Risk of flare-up was recorded by 8 studies (1110 teeth) and was significantly higher after single-visit versus multiple-visit treatment (RR 2.13 (95% CI 1.16 to 3.89); very weak evidence). Trial-sequential analysis revealed that firm evidence for benefit, harm or futility was not reached for any of the outcomes.
Conclusions: There is insufficient evidence to rule out whether important differences between both strategies exist.
Clinical significance: Dentists can provide root canal treatment in 1 or multiple visits. Given the possibly increased risk of flare-ups, multiple-visit treatment might be preferred for certain teeth (eg, those with periapical lesions).
Keywords: Clinical outcomes; Clinical studies/trials; Comparative effectiveness research (CER); Endodontics; Evidence-based dentistry/health care; Systematic reviews and evidence-based medicine.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Publication types
- Meta-Analysis
- Systematic Review
- Office Visits*
- Pain, Postoperative / etiology
- Randomized Controlled Trials as Topic
- Root Canal Therapy / adverse effects*
- Root Canal Therapy / methods*
- Symptom Flare Up
- Popular Professionals
- Design & Planning
- Construction & Renovation
- Finishes & Fixtures
- Landscaping & Outdoor
- Systems & Appliances
- Interior Designers & Decorators
- Architects & Building Designers
- Design-Build Firms
- Kitchen & Bathroom Designers
- General Contractors
- Kitchen & Bathroom Remodelers
- Home Builders
- Roofing & Gutters
- Cabinets & Cabinetry
- Tile & Stone
- Hardwood Flooring Dealers
- Landscape Contractors
- Landscape Architects & Landscape Designers
- Home Stagers
- Swimming Pool Builders
- Lighting Designers and Suppliers
- 3D Rendering
- Sustainable Design
- Basement Design
- Architectural Design
- Universal Design
- Energy-Efficient Homes
- Multigenerational Homes
- House Plans
- Home Remodeling
- Home Additions
- Green Building
- Garage Building
- New Home Construction
- Basement Remodeling
- Stair & Railing Contractors
- Cabinetry & Cabinet Makers
- Roofing & Gutter Contractors
- Window Contractors
- Exterior & Siding Contractors
- Carpet Contractors
- Carpet Installation
- Flooring Contractors
- Wood Floor Refinishing
- Tile Installation
- Custom Countertops
- Quartz Countertops
- Cabinet Refinishing
- Custom Bathroom Vanities
- Finish Carpentry
- Cabinet Repair
- Custom Windows
- Window Treatment Services
- Window Repair
- Fireplace Contractors
- Paint & Wall Covering Dealers
- Door Contractors
- Glass & Shower Door Contractors
- Landscape Construction
- Land Clearing
- Garden & Landscape Supplies
- Deck & Patio Builders
- Deck Repair
- Patio Design
- Stone, Pavers, & Concrete
- Paver Installation
- Driveway & Paving Contractors
- Driveway Repair
- Asphalt Paving
- Garage Door Repair
- Fence Contractors
- Fence Installation
- Gate Repair
- Pergola Construction
- Spa & Pool Maintenance
- Swimming Pool Contractors
- Hot Tub Installation
- HVAC Contractors
- Electricians
- Appliance Services
- Solar Energy Contractors
- Outdoor Lighting Installation
- Landscape Lighting Installation
- Outdoor Lighting & Audio/Visual Specialists
- Home Theater & Home Automation Services
- Handyman Services
- Closet Designers
- Professional Organizers
- Furniture & Accessories Retailers
- Furniture Repair & Upholstery Services
- Specialty Contractors
- Color Consulting
- Wine Cellar Designers & Builders
- Home Inspection
- Custom Artists
- Columbus, OH Painters
- New York City, NY Landscapers
- San Diego, CA Bathroom Remodelers
- Minneapolis, MN Architects
- Portland, OR Tile Installers
- Kansas City, MO Flooring Contractors
- Denver, CO Countertop Installers
- San Francisco, CA New Home Builders
- Rugs & Decor
- Home Improvement
- Kitchen & Tabletop
- Bathroom Vanities
- Bathroom Vanity Lighting
- Bathroom Mirrors
- Bathroom Fixtures
- Nightstands & Bedside Tables
- Kitchen & Dining
- Bar Stools & Counter Stools
- Dining Chairs
- Dining Tables
- Buffets and Sideboards
- Kitchen Fixtures
- Wall Mirrors
- Living Room
- Armchairs & Accent Chairs
- Coffee & Accent Tables
- Sofas & Sectionals
- Media Storage
- Patio & Outdoor Furniture
- Outdoor Lighting
- Ceiling Lighting
- Chandeliers
- Pendant Lighting
- Wall Sconces
- Desks & Hutches
- Office Chairs
- View All Products
- Designer Picks
- Side & End Tables
- Console Tables
- Living Room Sets
- Chaise Lounges
- Ottomans & Poufs
- Bedroom Furniture
- Nightstands
- Bedroom Sets
- Dining Room Sets
- Sideboards & Buffets
- File Cabinets
- Room Dividers
- Furniture Sale
- Trending in Furniture
- View All Furniture
- Bath Vanities
- Single Vanities
- Double Vanities
- Small Vanities
- Transitional Vanities
- Modern Vanities
- Houzz Curated Vanities
- Best Selling Vanities
- Bathroom Vanity Mirrors
- Medicine Cabinets
- Bathroom Faucets
- Bathroom Sinks
- Shower Doors
- Showerheads & Body Sprays
- Bathroom Accessories
- Bathroom Storage
- Trending in Bath
- View All Bath
- Houzz x Jennifer Kizzee
- Houzz x Motivo Home
- How to Choose a Bathroom Vanity

- Patio Furniture
- Outdoor Dining Furniture
- Outdoor Lounge Furniture
- Outdoor Chairs
- Adirondack Chairs
- Outdoor Bar Furniture
- Outdoor Benches
- Wall Lights & Sconces
- Outdoor Flush-Mounts
- Landscape Lighting
- Outdoor Flood & Spot Lights
- Outdoor Decor
- Outdoor Rugs
- Outdoor Cushions & Pillows
- Patio Umbrellas
- Lawn & Garden
- Garden Statues & Yard Art
- Planters & Pots
- Outdoor Sale
- Trending in Outdoor
- View All Outdoor
- 8 x 10 Rugs
- 9 x 12 Rugs
- Hall & Stair Runners
- Home Decor & Accents
- Pillows & Throws
- Decorative Storage
- Faux Florals
- Wall Panels
- Window Treatments
- Curtain Rods
- Blackout Curtains
- Blinds & Shades
- Rugs & Decor Sale
- Trending in Rugs & Decor
- View All Rugs & Decor
- Pendant Lights
- Flush-Mounts
- Ceiling Fans
- Track Lighting
- Wall Lighting
- Swing Arm Wall Lights
- Display Lighting
- Table Lamps
- Floor Lamps
- Lamp Shades
- Lighting Sale
- Trending in Lighting
- View All Lighting
- Bathroom Remodel
- Kitchen Remodel
- Kitchen Faucets
- Kitchen Sinks
- Major Kitchen Appliances
- Cabinet Hardware
- Backsplash Tile
- Mosaic Tile
- Wall & Floor Tile
- Accent, Trim & Border Tile
- Whole House Remodel
- Heating & Cooling
- Building Materials
- Front Doors
- Interior Doors
- Home Improvement Sale
- Trending in Home Improvement
- View All Home Improvement
- Cups & Glassware
- Kitchen & Table Linens
- Kitchen Storage and Org
- Kitchen Islands & Carts
- Food Containers & Canisters
- Pantry & Cabinet Organizers
- Kitchen Appliances
- Gas & Electric Ranges
- Range Hoods & Vents
- Beer & Wine Refrigerators
- Small Kitchen Appliances
- Cookware & Bakeware
- Tools & Gadgets
- Kitchen & Tabletop Sale
- Trending in Kitchen & Tabletop
- View All Kitchen & Tabletop
- Storage & Organization
- Baby & Kids
- Housekeeping & Laundry
- Pet Supplies

- View all photos
- Dining Room
- Breakfast Nook
- Family Room
- Bed & Bath
- Powder Room
- Storage & Closet
- Outdoor Kitchen
- Bar & Wine
- Wine Cellar
- Home Office
- Popular Design Ideas
- Kitchen Backsplash
- Deck Railing
- Privacy Fence
- Small Closet
- Stories and Guides
- Popular Stories
- Renovation Cost Guides
- Fence Installation Cost Guide
- Window Installation Cost Guide
- Discussions
- Design Dilemmas
- Before & After
- Houzz Research
- View all pros
- View all services
- View all products
- View all sales
- Living Room Chairs
- Dining Room Furniture
- Coffee Tables
- Home Office Furniture
- Join as a Pro
- Interior Design Software
- Project Management
- Custom Website
- Lead Generation
- Invoicing & Billing
- Landscape Contractor Software
- General Contractor Software
- Remodeler Software
- Builder Software
- Roofer Software
- Architect Software
- Takeoff Software
- Lumber & Framing Takeoffs
- Steel Takeoffs
- Concrete Takeoffs
- Drywall Takeoffs
- Insulation Takeoffs
- Stories & Guides
- LATEST FROM HOUZZ
- HOUZZ DISCUSSIONS
- SHOP KITCHEN & DINING
- Kitchen & Dining Furniture
- Sinks & Faucets
- Kitchen Cabinets & Storage
- Knobs & Pulls
- Kitchen Knives
- KITCHEN PHOTOS
- FIND KITCHEN PROS
- Bath Accessories
- Bath Linens
- BATH PHOTOS
- FIND BATH PROS
- SHOP BEDROOM
- Beds & Headboards
- Bedroom Decor
- Closet Storage
- Bedroom Vanities
- BEDROOM PHOTOS
- Kids' Room
- FIND DESIGN PROS
- SHOP LIVING
- Fireplaces & Accessories
- LIVING PHOTOS
- SHOP OUTDOOR
- Pool & Spa
- Backyard Play
- OUTDOOR PHOTOS
- FIND LANDSCAPING PROS
- SHOP LIGHTING
- Bathroom & Vanity
- Flush Mounts
- Kitchen & Cabinet
- Outdoor Wall Lights
- Outdoor Hanging Lights
- Kids' Lighting
- Decorative Accents
- Artificial Flowers & Plants
- Decorative Objects
- Screens & Room Dividers
- Wall Shelves
- About Houzz
- Houzz Credit Cards
- Privacy & Notice
- Cookie Policy
- Your Privacy Choices
- Mobile Apps
- Copyright & Trademark
- For Professionals
- Houzz vs. Houzz Pro
- Houzz Pro vs. Ivy
- Houzz Pro Advertising Reviews
- Houzz Pro 3D Floor Planner Reviews
- Trade Program
- Buttons & Badges
- Your Orders
- Shipping & Delivery
- Return Policy
- Houzz Canada
- Review Professionals
- Suggested Professionals
- Accessibility
- Houzz Support
- COUNTRY COUNTRY
New & Custom Home Builders in Elektrostal'
Location (1).
- Use My Current Location
Popular Locations
- Albuquerque
- Cedar Rapids
- Grand Rapids
- Indianapolis
- Jacksonville
- Kansas City
- Little Rock
- Los Angeles
- Minneapolis
- New Orleans
- Oklahoma City
- Orange County
- Philadelphia
- Portland Maine
- Salt Lake City
- San Francisco
- San Luis Obispo
- Santa Barbara
- Washington D.C.
- Elektrostal', Moscow Oblast, Russia
Professional Category (1)
- Accessory Dwelling Units (ADU)
Featured Reviews for New & Custom Home Builders in Elektrostal'
- Reach out to the pro(s) you want, then share your vision to get the ball rolling.
- Request and compare quotes, then hire the Home Builder that perfectly fits your project and budget limits.
Before choosing a Builder for your residential home project in Elektrostal', there are a few important steps to take:
- Define your project: Outline your desired home type, features, and layout. Provide specific details and preferences to help the builder understand your vision.
- Establish a budget: Develop a comprehensive budget, including construction expenses and material costs. Communicate your budgetary constraints to the builder from the beginning.
- Timeline: Share your estimated timeline or desired completion date.
- Site conditions: Inform the builder about any unique site conditions or challenges.
- Local regulations: Make the builder aware of any building regulations or permits required.
- Land Surveying
What do new home building contractors do?
Questions to ask a prospective custom home builder in elektrostal', moscow oblast, russia:.
If you search for Home Builders near me you'll be sure to find a business that knows about modern design concepts and innovative technologies to meet the evolving needs of homeowners. With their expertise, Home Builders ensure that renovation projects align with clients' preferences and aspirations, delivering personalized and contemporary living spaces.
BUSINESS SERVICES
Connect with us.
IMAGES
VIDEO
COMMENTS
For risk of long-term complications, we did not find a difference between single-visit and multiple-visit endodontic treatment. This was our primary outcome as such complications oftentimes decide the fate of the tooth. 56-58 It is noteworthy that this was supported by a range of studies (ie, studies with high or low risk, ...
Single-visit endodontics is defined as "the conservative. non -surgical treatment of an endodontically involved tooth consisting of complete biomechanical cleansing, shaping, and obturation. of ...
Single-visit endodontic therapy is an old concept in clinical practice. However, the controversy still exists as to which root canal treatment option is best between single- and multiple-visit ...
Objectives Single-visit root canal treatment has some advantages over conventional multivisit treatment, but might increase the risk of complications. We systematically evaluated the risk of complications after single-visit or multiple-visit root canal treatment using meta-analysis and trial-sequential analysis. Data Controlled trials comparing single-visit versus multiple-visit root canal ...
Single visit endodontic therapy: Omar Ikram Much time has been spent investigating and researching the healing or maintenance of periapical health, commonly called 'success', of single visit versus multiple visit root canal treatment. The consensus is that there is no significant difference in success rates of either
Single- visit endodontic therapy is defined as "the conservative and nonsurgical root canal. treatment of an involved tooth consisting of complete chemomechanical preparation and. obturation of ...
The Science of Single-Visit Endodontics: Apical Sizes Revisited. Recent studies support larger apical preparation sizes to remove more infected tissue and bacteria10-13 and provide more canal space for more effective irrigation.14 Simply stated, preparing canals to larger apical sizes is the right thing to do, especially if single-visit ...
The advantages, disadvantages, safety, and effectiveness of endodontic treatment in a single visit compared with the multiple-visit approach were investigated in SRs 4, 7, 8. SRs include scientific evidence from different primary studies including randomized clinical trials and prospective and retrospective designs. Consequently, this overview ...
To achieve this, endodontic therapy used to be performed in multiple visits for complete disinfection of the canals in other words for the better success of endodontic therapy. 1 One-visit endodontic therapy is defined as 'the conservative non-surgical treatment of an endodontically involved tooth consisting of complete biomechanical ...
146 Myths associated with single visit endodontics There are three major reasons that patients once refused endodontic treatment and often chose tooth extraction instead: cost, fear of pain, and time.
Single visit versus multiple visit root canal. Assessment of the preference of single visit over multiple visit root canals shows that people between 26 to 45 years are often affected with dental caries, and available data is biased towards multi visits rather than single visit regardless number of canals. Expand.
Objectives: Single-visit root canal treatment has some advantages over conventional multivisit treatment, but might increase the risk of complications. We systematically evaluated the risk of complications after single-visit or multiple-visit root canal treatment using meta-analysis and trial-sequential analysis. ... Endodontics; Evidence-based ...
629 likes, 20 comments - abdulwahab.alqaraghuli on May 10, 2024: "Single Visit RCT for Curvy Premolar Obturation with EndoSeal BC frim maruchi #endo #endodontia #endodontics#endodoncia #dentistry #d ...
Single-visit endodontic treatment and multiple-visit endodontic treatment both have their advantages and disadvantages. This paper is a literature review of the research on nonsurgical single-visit versus multiple-visit endodontic treatment. The PubMed database was searched using the keywords (endodontic treatment OR endodontic therapy OR root ...
In 1938, it was granted town status. [citation needed]Administrative and municipal status. Within the framework of administrative divisions, it is incorporated as Elektrostal City Under Oblast Jurisdiction—an administrative unit with the status equal to that of the districts. As a municipal division, Elektrostal City Under Oblast Jurisdiction is incorporated as Elektrostal Urban Okrug.
Moscow Oblast (Russian: Московская область, romanized: Moskovskaya oblast, IPA: [mɐˈskofskəjə ˈobləsʲtʲ], informally known as Подмосковье, Podmoskovye, IPA: [pədmɐˈskovʲjə]) is a federal subject of Russia (an oblast).With a population of 8,524,665 (2021 Census) living in an area of 44,300 square kilometers (17,100 sq mi), it is one of the most densely ...
Single visit endodontic treatment had numerous drawbacks primarily about the post-operative pain. and failure of the treatment effect. With recent adv ances in endodontics the single visit therapy ...
Its a city in the Moscow region. As much effort they take in making nice flags, as low is the effort in naming places. The city was founded because they built factories there.
Search 1,121 Elektrostal' new & custom home builders to find the best custom home builder for your project. See the top reviewed local custom home builders in Elektrostal', Moscow Oblast, Russia on Houzz.